 Print
PrintTreatments
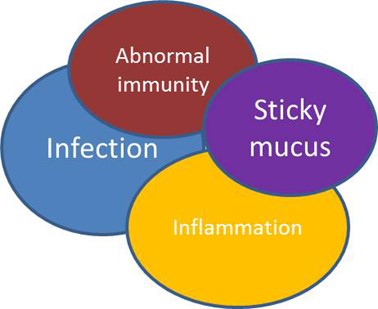
This diagram shows the problems that contribute to the symptoms of bronchiectasis. They are all linked together: Having sticky mucus that is difficult to clear from your chest will lead to more infections and inflammation in the lungs. If your immune system is not working properly you will also be prone to infections.
- To treat bronchiectasis, different treatments are needed to work on each of these factors.
- Treatments will differ between people depending on which aspects cause most of a problem for them.
- For example, to help with mucus clearance, tablets that make the mucus thinner and easier to cough up can be used, and physiotherapy is very important to help to clear the mucus from your lungs.
Antibiotics
Antibiotics are needed for 14 days when you have a chest infection, flare-up or exacerbation of bronchiectasis.
The antibiotics used will vary depending on which bugs there are in your sputum. This is why it is important to give a phlegm sample when you notice things changing, so that your doctor knows which antibiotics would be best for you to have. You can then start a course of antibiotics without having to wait for the results. Often antibiotic choice will be guided by what bugs you have had in the past or which antibiotics have worked best for you in the past. If the results show a new bug or a bug that will not be treated by the antibiotics you have started, your doctor may prescribe a different antibiotic.
It is important that you play an active role in putting in a sputum sample early, and telling your doctor which treatments work best for you.
Sometimes, antibiotics are also used long-term, not just for a 2 week course. These include a tablet called azithromycin, and nebulised antibiotics such as gentamicin and colomycin.
More details can be found below
Antibiotic tablets
- Standard antibiotics for flare-ups or chest infections in bronchiectasis tend to be:
- Amoxicillin 500mg three times a day for 14 days or Clarithromycin 500mg twice a day for 14 days if you are allergic to penicillin.
- Other tablet antibiotics frequently used for flare-ups include doxycycline and ciprofloxacin. Ciprofloxacin tends to be used if you have the bug Pseudomonas aeruginosa in your phlegm. There are other tablets that are used depending on the bugs in your sputum.
- If you are having more than 3 courses of antibiotics in a year, your doctor may recommend trying a tablet called azithromycin. This is an antibiotic that also reduces inflammation in the lungs. It is usually taken 3 times a week (mon/weds/fri) and you may stay on this long-term. If you are on this tablet you will need to have regular liver blood tests and mention any hearing problems to your doctor.
Click here to see more information about azithromycin
- Another way of taking long-term antibiotics is by nebuliser.
Nebulised antibiotics
- If you have more than 3 infections per year requiring antibiotics, have lots of troublesome sputum or if the bug pseudomonas aeruginosa is repeatedly grown from your sputum samples, having long term antibiotics via a nebuliser may be an option.
- Antibiotics that are given through a nebuliser commonly include gentamicin and colomycin.
- More details can be found in the nebulised treatments and microbiology sections.
Antibiotics into veins (intravenous/IV)
Sometimes you might need IV antibiotics if you are very unwell or if you have an infection that does not respond to tablet antibiotics.
Having IVs in hospital
- Some people come into hospital for their IV antibiotics and stay there while they have the course of treatment (usually 2 weeks).This may be because you’re unwell or don’t have the support to continue your treatment at home. In this case, hospital is the safest place to be. Often being in a place of safety and having the opportunity to rest and recover will enhance your recovery from a flare up of bronchiectasis
- In additional to your IV antibiotics treatment, you will also meet a range of health professionals who can help you with your disease. These will include doctors, nurses, physiotherapists, dieticians and other members of staff.
Having IVs at home
- You may be able to have IV antibiotics at home. You or your family member can be trained to prepare and give IV antibiotics. This will depend on whether your medical team are able to offer this service. If they are, they will make sure that you have the right training, education and support in order to be able to do this. They will also offer a point of contact at the hospital in case you have any problems when you are at home. Usually you will be in hospital for a short time and then continue the course at home.
- If you don't feel confident doing this yourself at home, some community teams have nurses who have the skills to help. Unfortunately, not all areas currently offer this service. Please speak to hospital staff to see if this is an option.
"I’m quite confident now. At first it’s nerve-wracking trying to remember what to do but when I had finished his fortnight I was quite confident…the nurse is very helpful, and I’ve got a sheet of paper telling me exactly what to do, so I was quite confident really when I started them." Elaine, 68
IV antibiotics can be given by:
- Cannula: a small plastic tube inserted into a vein in your arm. The IV antibiotics are given directly into this. A cannula usually needs to be changed every 3 days for infection control reasons.
- Midline catheter: a very thin tube, longer than a cannula, which is also inserted into a vein in your arm. This is done on the ward by a very experienced nurse or doctor and is a much safer way of giving your IV antibiotics. A midline is more comfortable and can also stay in the arm for the duration of the treatment and does not need to be changed.
- Portacath: a small device which is inserted under the skin in your chest. This is performed by a radiology doctor in the x-ray department. A tube connects the portacath to your veins. When you need IV antibiotics an experienced nurse will insert a special needle into this portacath and secure it with a dressing. This special needle then stays in for the course of the treatment. When the treatment is finished the needle is removed. We generally reserve portacaths for people with difficult veins or those who require frequent courses of IV antibiotics. Portacaths can stay in place for many years and complications are rare.
Click here to see how to give IV Ceftazadime
Click here to see a Home IV Instruction Manual
ALWAYS GIVE A SPUTUM SAMPLE BEFORE STARTING A COURSE OF ANTIBIOTICS
Nebulised treatments
- Nebulised treatments involve converting a liquid into a mist which you can then breathe in. By aiming the treatment directly at your lungs we can minimise any side effects.
- Nebulised treatments can cause you to have some wheezing or cough either on commencement of the treatment or after a period of a few weeks.
- Patients go into hospital to commence the treatment and staff will measure your breathing tests and monitor you to make sure that the treatment is right for you.
- A number of different nebulisers are available. The hospital are likely to give you a standard nebuliser, but smaller, faster versions are available that you may find easier to travel with for example.
- Nebulisers take up a certain amount of your time – both to prepare and inhale the treatment, and to clean the nebuliser afterwards.
“And it’s absolutely fantastic, the difference it’s made to me. It is a nuisance, the nebuliser, yes. But, my quality of life has changed … When it was recommended I use it and I will find the benefits of it, I was all doom and gloom…I was shocked, I was in horror about it. But it was because of ignorance, I thought that was the end, but it hasn’t been. You know it’s a pain, it takes an hour of your day up. But you are gaining the benefits.” Mavis, 62
A number of different treatments can be given via a nebuliser. In bronchiectasis the most commonly used are:
Nebulised Antibiotics
- Colomycin and gentamicin are the most commonly used nebulised antibiotics in bronchiectasis. This involves inhaling a fine mist of liquid antibiotics which can be breathed in through a mouthpiece.
- Your doctor may suggest that you try these if for example you are having lots of chest infections or flare ups, have lots of troublesome sputum or if you have particular bugs such as pseudomonas aeruginosa. The aim of the treatment is to reduce the number of flare ups you have been having and to improve your symptoms. Some people feel that the volume of sputum is reduced whilst on inhaled antibiotics. You may have a trial for a few months at first, and then continue long-term if you have had improvements in your symptoms.
- If you are starting a new nebulised treatment, you will have a test dose at the hospital first. This is to make sure that you know how to do the treatment and that you do not have any reactions to it. Occasionally inhaling treatments can make some people wheezy. If this is a particular problem for you, you may have to try alternative treatments.
Click here for more information about nebulised gentamicin.
Click here for more information and nebulised colomycin.
Nebulised hypertonic saline (salty water)
- This is a strong salt solution which is used in a nebuliser. This is something your doctor may suggest trying if you are having frequent infections or have difficulty clearing sputum from your lungs when doing physiotherapy. Using this treatment can help to break the phlegm up and make it easier to cough. We normally prescribe it twice a day.
- Some patients use it twice a day when their phlegm is sticky or if they are unwell. When they are feeling better, or their sputum is less sticky, they may reduce the frequency.
- When you first start you will have a test dose in hospital and have your breathing tests checked before and afterwards. This is because it can make some people breathless and we need to check that this is not a problem for you.
- Click on these links to get more information about hypertonic saline.
Inhalers
- Sometimes inhalers are used in bronchiectasis.
- Although bronchiectasis is NOT the same as asthma or COPD (smoking related lung damage), some of the ways the lungs are affected are similar.
- This means that for some people, inhalers can be useful.
- These may include ‘relievers’ (salbutamol), which act to open up the airways, relieving breathlessness on exertion.
- Some inhalers contain a small dose of steroid, which acts to reduce inflammation in the airways (beclometasone) and are usually used in asthma. Evidence from studies in bronchiectasis only supports the use of these inhalers in bronchiectasis if there are some asthma symptoms too.
- Other inhalers contain a combination of a steroid and an airway opener, such as symbicort or seretide. Although these are not routinely used in all patients with bronchiectasis, they are sometimes used.
- The decision to use inhalers will be based upon your symptoms, your medical history and your breathing test results.
- If you do take inhalers it is very important that you follow the correct procedure for taking them.
Here are some links to see videos about how to use your inhalers
How to use an accuhaler (seretide)
How to use a turbohaler (symbicort)
How to use a metered dose inhaler
How to use a metered dose inhaler with a spacer
How to use an easi-breathe inhaler
Mucus (phlegm) thinning tablets
- A tablet called carbocisteine or Mucodyne is sometimes used to help make sputum (phlegm or mucus) easier to clear from your lungs.
- This is something that your doctor may suggest if you have difficulty clearing your chest.
- Clearing phlegm from your lungs is very important in bronchiectasis and can reduce the number of infections that you have.
Mucus (phlegm) clearance
- This is extremely important for people who have bronchiectasis.
- Performing chest physiotherapy is essential to clear your chest.
Physiotherapy
Why do I need physiotherapy?
- Bronchiectasis can cause mucus to collect in the lungs and become infected.
- As a result of this you will be more susceptible to chest infections than other people. You may also have a persistent cough.
- Each time you get a chest infection it can cause a little more damage and scarring to the lungs.
- You may find that with these problems you get more breathless and can lose fitness.
How can physiotherapy help me?
- Your respiratory physiotherapist will teach you airway clearance techniques to do daily at home.
- This is to help keep your chest clear of sputum so that your condition impacts you as little as possible on your everyday life.
- It will also help with the persistent cough that many people have.
- It is very important to keep fit so that you remain as well as possible. See ‘diet exercise and lifestyle advice’. There are also techniques to help with managing breathlessness.
What will this physiotherapy be?
- Your physiotherapist will need to fully assess you. He or she will ask you questions about your symptoms and your sputum, and will examine your chest.
- You will then discuss options of different methods to help you remove the sputum from your lungs.
- Your physiotherapist will help you choose the airway clearance technique that is most suited to you and your particular needs, and recommend how often you should perform them.
How will I know if my regular chest physiotherapy is not enough or if I should change my treatment?
- If the method you use to clear your chest is not working for you, if you have difficulty in clearing your sputum, or you are not comfortable with the technique, contact your physiotherapist about trying a different one.
- At times when you have a chest infection you may also need to change or add to your treatment.
Please see the additional sections relating to this for more information and videos:
Treatments less frequently used
Surgery and embolisation
-
In the past, surgery was more often performed for people who had bronchiectasis in a particular lung segment. This would involve that section of the lung being removed. We now know that this is not often helpful, and so surgery is very rarely performed in bronchiectasis any more.
-
Sometimes people can have a problem with coughing blood. If this is a problem for you then you may have a specific type of scan called pulmonary angiography to look at the blood vessels in the lungs. If there are vessels that can be seen to be the cause of the bleeding then this can be helped by a procedure called embolisation where the blood vessel(s) causing the trouble are blocked off, and occasionally by surgery to remove the area of lung with abnormal vessels and bleeding.
Lung Transplantation
- Lung transplantation is again rarely needed in bronchiectasis.
- In certain circumstances, this may be thought to be a suitable treatment. This is reserved for people who have very severe lung disease and no other treatment options. They would also have to be otherwise healthy and meet certain other criteria.
- This is a very complex process, but if your doctor thinks it may be the best treatment for you then they will discuss this with you.
The British Lung Foundation can provide more information about lung transplantation.
Oxygen
- Occasionally, people who have severe lung disease of any kind, require oxygen to be used at home.
- When you attend clinic and have breathing tests done, your oxygen saturation levels are also checked. If your oxygen falls below a certain level, then you may need to be assessed for home oxygen use.
The British Lung Foundation can provide more information about oxygen.

